TL;DR. A world first: a humanoid companion robot inside the pediatric radiotherapy journey at the ICM Montpellier. Not to heal. So that no child is ever alone inside a bunker. 14 children followed, 172 documented interactions, an international dosimetric validation. The story started with a five-year-old girl strapped to a treatment table, and with a Japanese robot that handed me a towel on a rainy day.
Charline
I’ve been a radiation oncologist for seven years. I’ve treated children aged 3 to 18, brain tumors, leukemias, sarcomas. Every year in the world, 400,000 children are diagnosed with cancer, and a third of them receive radiotherapy.
And then there was Charline.
Charline was five years old. She cried every day, at every session.
She needed more than an hour to complete a treatment that should have lasted ten minutes. Tears for her. Tears for her mother, for her father. And an infinite sadness for us, the caregivers, watching her from behind the bunker door without being able to do anything.
The beam is too powerful. Nobody can enter the bunker during irradiation. Not the mother, not the father, not the doctor. Nobody.
Charline stayed alone in that reinforced-concrete room while the machine rotated above her.
I felt so powerless, unable to support her beyond the threshold of the bunker. One question stayed planted in me: what can I do?

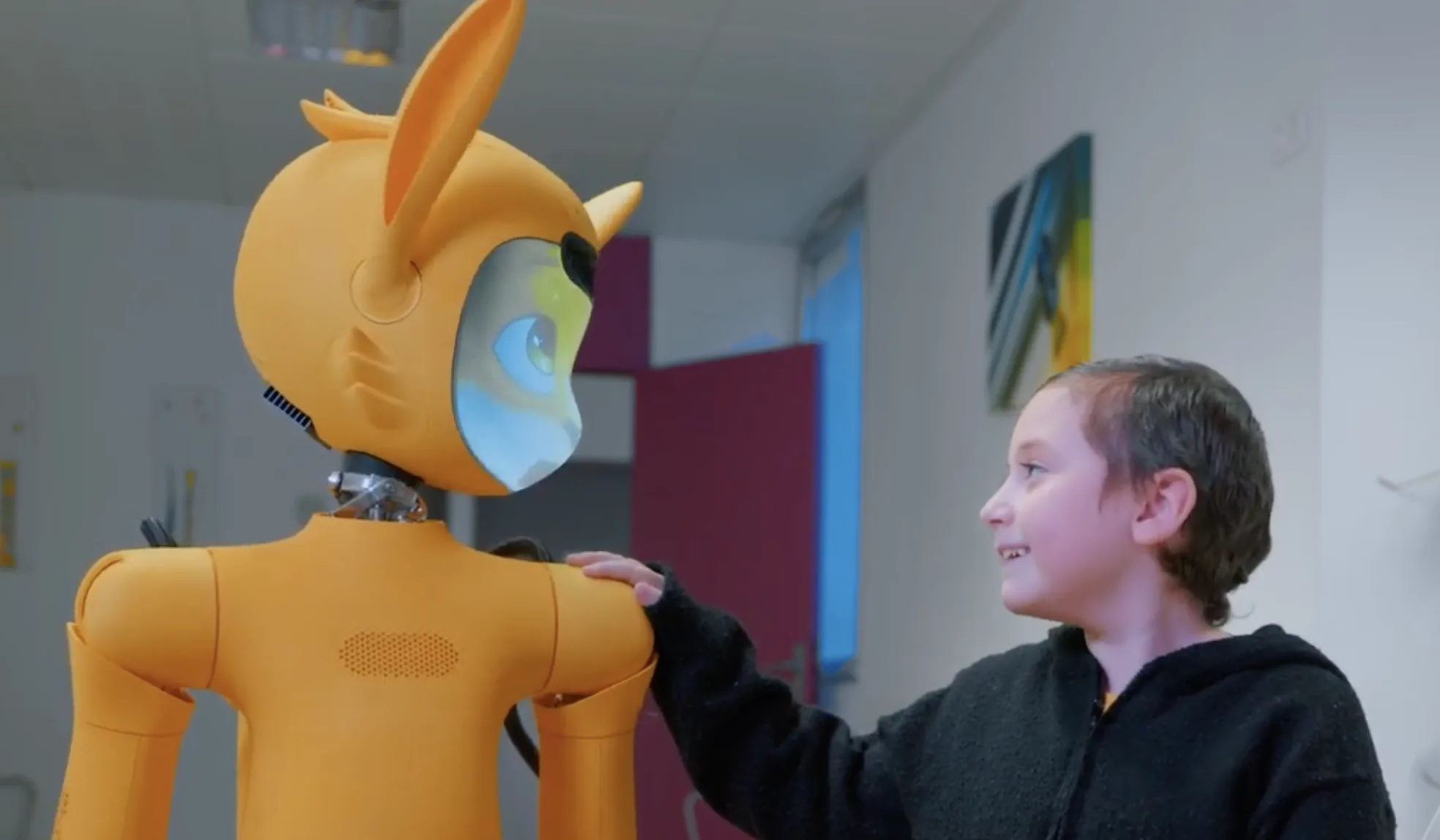
Miroki in the treatment room at the ICM Montpellier. The bunker is no longer an empty room.
The problem we don’t talk about
In radiotherapy, from a physician’s standpoint, the beauty of the gesture is precision. We target the tumor to the millimeter while sparing healthy tissue around it. It’s high-precision engineering.
From the child’s standpoint, it’s something else.
It’s a daily obligation. You come every day, twenty minutes, for one to two months. Under a big machine. Sometimes the skin burns. You know you have a tumor inside your body trying to kill you, and you still have to come.
The room is dark, no window, thick walls. A printed sky on a false ceiling reduces anxiety by almost 20% according to studies. That’s the best we had for years.
You lie down on the black table, the machine moves around you without touching you. For an adult, it’s already hard. For a child, it’s terror.
And the terror has a very concrete consequence: if the child moves, the dose shifts. A dose that shifts means a lifelong side effect. So we must guarantee immobility.
The standard solutions are general anesthesia or physical restraint. Neither is neutral. Neither solves the real problem, which is not immobility. The real problem is that the child is alone.
For a long time, I told myself we just had to accept this. This was medicine, this was how it worked.
And then I went to Japan…
Tokyo, the rain, a towel
It was a trip to Japan, I love that country. A day of pouring rain. I was soaked, I took shelter in a store.
And a robot came toward me.
It rolled forward, handed me a towel, smiling.
I stayed there, the towel in my hand. Wow, that’s useful.
And suddenly, I thought of Charline.
If a robot could roll toward me to hand me a towel when I was wet, could a robot keep a five-year-old company in a room where nobody was allowed to enter?
The idea flipped in one breath. The robot became the missing piece of the journey: the only entity that could cross the bunker door during irradiation. Not to heal. Just to be there.
I started looking.
Every robot, every stat, every possibility. Comparisons, tech sheets, demos. For months.
And one day, I found my robot. Miroki, designed by Enchanted Tools, a young French startup. Back then, it couldn’t even talk yet.
I contacted them and I said: I want this robot, for my little patients.
Miroki, the answer
It became the Miroki project, at the ICM Montpellier. From the Japanese miru (見る), to see. To see without healing. To be there without imposing.
Miroki has evolved a lot in a year. He walks, he dances, he catches, he speaks. Above all, he has a story, a narrative universe. Children love stories. We all do, really.
We designed a three-step care journey, built so that the relationship between the child and the robot would form before the very first session.
Step 1, the consultation. Miroki waits for the child and the parents at the end of the announcement consultation. The child meets him in person for the first time. Just a meeting.
Step 2, the preparation. Before radiotherapy, there are several technical steps (simulation scan, positioning, fabrication of a thermoformed mask for brain tumors). Miroki goes with the child to each of them, so the bond strengthens.
Step 3, the treatment. The child and Miroki have grown close. Miroki is perceived as a real companion. And he enters with the child into the treatment room. The child is no longer alone.
After every interaction, a report is generated for the medical team. How the child reacted, what they said, what worked and what didn’t. We stop losing information between sessions.
Beyond the robot, there is a research protocol: KOKORO, carried by the SIRIC Montpellier Cancer. Kokoro (心) in Japanese means the heart. But also the mind, the intention, what animates. The idea: measure what had never been measured until now. The anxiety level, the quality of cooperation, the real need for general anesthesia.
Quantify the unquantifiable. To be able to defend it in front of teams, funders, ethics committees.
Miroki isn’t a robot that heals. It heals something else: it makes human again what had stopped being so.
Georgia, and the proof
After a year, we have 14 children documented. 172 recorded interactions. And one case that changes everything.
Georgia, 8 years old. First patient accompanied all the way into the irradiation room with confirmed dosimetric validation.
Georgia, 8 years old.
First patient accompanied all the way into the irradiation room with confirmed dosimetric validation. Concretely: Miroki entered the bunker during a real session, without disturbing the dose, without degrading the precision of the treatment. The report was submitted to an international review in July 2025.
To anyone outside radiotherapy, this sounds anecdotal. To anyone inside, it’s a tremor.
Before Georgia, the idea of a robot inside a bunker during irradiation made medical physicists smile. Too many uncertainties, too much matter in the beam, too many risks.
After Georgia, it became defensible. A protocol, a publication, a precedent.
For Georgia herself, it was mostly her session, calmer, without restraint, without tears. A session where she wasn’t alone.
What we learned that year wasn’t that technology could replace a caregiver. It was that technology could be there when the caregiver physically could not.
What really struck me wasn’t the technical achievement. It was the question that imposed itself on me as cases piled up. If we had missed all that in pediatric radiotherapy, what were we missing elsewhere in care when we looked only at biology?
What a robot can be
A robot is not a caregiver. It will never hold a diploma, it will never take a medical decision, it will never replace the presence of a mother, a father, a technologist who knows the child by name. Pretending otherwise would be naive, and letting it be implied would be dangerous.
But it can be there. Just that. Be there, in a room where nobody else is allowed to enter. Without intent, without prescription, without clinical target. A humble presence that means the child is no longer alone.
For a long time, we thought technology always had to add something. Intelligence, performance, speed. Miroki taught me it can also, sometimes, simply hold a place. The one no human can hold. Behind Georgia, there are tens of thousands of children each year crossing a radiotherapy bunker around the world. Behind each of them, the same empty room, the same closed door, the same question.
This isn’t a revolution. It’s a gap we had learned to accept.
What it opens
Miroki isn’t an end. It’s the first piece of a larger puzzle.
During those years with him, I didn’t just watch a robot interact with children. I observed. I took notes. I read. Developmental psychology, theory of mind, human-machine interaction, affective robotics, non-verbal communication, behavioral science. Books piled on my bedside table, annotated papers, conversations with researchers and caregivers from other disciplines. I was trying to understand what Miroki was doing right, what other AIs were doing wrong, and why.
That synthesis work, I accelerated it over the last few years with AI. In parallel to the Miroki project, I built a personal system of capture, indexing, and cross-linking for everything I read, meet, observe. An augmented memory that absorbs my sources, compares my notes, links my intuitions, challenges my conclusions. Without that system, this article might still have existed. But the density of what I’ve been able to connect in so little time wouldn’t have.
What this experience taught me is that the AIs and the robots we deploy in healthcare almost never fail on medical competence. They fail on behavioral competence: the ability to adapt the tone, the rhythm, the presence, to the actual state of a patient at a specific moment. The ability to speak caregiver.
That competence is what I’ll explore here, article by article. How it’s defined, how it’s taught, how it’s evaluated. I call it behavioral AI in care. It’s the thread of this series.
The next article will lay the frame: why most clinical AIs fail at the patient’s bedside, and what changes when we take behavior seriously.
In short, no child should ever be alone inside a bunker.
Technology may have finally found its rightful place. Not to replace the caregiver. To be there when the caregiver cannot be. And to leave, at the end of a session, a child who will remember having had someone beside them.
For my perspective on the future of humanoid robotics in healthcare, I wrote an article that crosses the 2026 global state of the art with fourteen months of observing Miroki at Montpellier Cancer Institute → Humanoid care robotics: what the research says, and what we see at Montpellier Cancer Institute with Miroki.
If you want to follow what comes next: the project page lives here → Miroki. The daily probes and raw thoughts on X → @JulienWelmant. And if you’re working on healthcare tools, or if you’re a patient who ever felt alone in a treatment room, write to me. That’s exactly why I started telling the story.